Herpes Support Group for Ladies - click this link
Herpes simplex - wikipedia part 1
Source:
http://en.wikipedia.org/wiki/Herpes_simplex
Herpes simplex (Ancient Greek: ἕρπης - herpes, lit. "creeping") is a viral disease caused by both herpes simplex virus type 1 (HSV-1) and type 2 (HSV-2). Infection with the herpes virus is categorized into one of several distinct disorders based on the site of infection. Oral herpes, the visible symptoms of which are colloquially called cold sores or fever blisters, infects the face and mouth. Oral herpes is the most common form of infection. Genital herpes, known simply as herpes, is the second most common form of herpes. Other disorders such as herpetic whitlow, herpes gladiatorum, ocular herpes (keratitis), cerebral herpes infection encephalitis, Mollaret's meningitis, neonatal herpes, and possibly Bell's palsy are all caused by herpes simplex viruses.
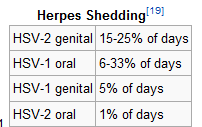
Herpes viruses cycle between periods of active disease—presenting as blisters containing infectious virus particles—that last 2–21 days, followed by a remission period. Genital herpes, however, is often asymptomatic, though viral shedding may still occur. After initial infection, the viruses are transported along sensory nerves to the sensory nerve cell bodies, where they become latent and reside life-long. Causes of recurrence are uncertain, though some potential triggers have been identified, including immunosuppressant drugs (see below). The previously latent virus then multiplies new virus particles in the nerve cell and these are transported along the axon of each neuron to the nerve terminals in the skin, where they are released. Over time, episodes of active disease reduce in frequency and severity.
Herpes simplex is most easily transmitted by direct contact with a lesion or the body fluid of an infected individual. Transmission may also occur through skin-to-skin contact during periods of asymptomatic shedding. Barrier protection methods are the most reliable method of preventing transmission of herpes, but they merely reduce rather than eliminate risk. Oral herpes is easily diagnosed if the patient presents with visible sores or ulcers. Early stages of orofacial herpes and genital herpes are harder to diagnose; laboratory testing is usually required.
A cure for herpes has not yet been developed. Once infected, the virus remains in the body for life. However, after several years, some people will become perpetually asymptomatic and will no longer experience outbreaks, though they may still be contagious to others. Treatments with antivirals can reduce viral shedding and alleviate the severity of symptomatic episodes. Vaccines are in clinical trials but have not demonstrated effectiveness. It should not be confused with conditions caused by other viruses in the herpesviridae family such as herpes zoster, which is caused by varicella zoster virus. The differential diagnosis includes hand, foot and mouth disease due to similar lesions on the skin.
Classification
Herpes simplex is divided into two types: HSV type 1 and HSV type 2. HSV1 primarily causes mouth, throat, face, eye, and central nervous system infections, while HSV2 primarily causes anogenital infections.[1] However, each may cause infections in all areas.
Signs and symptoms
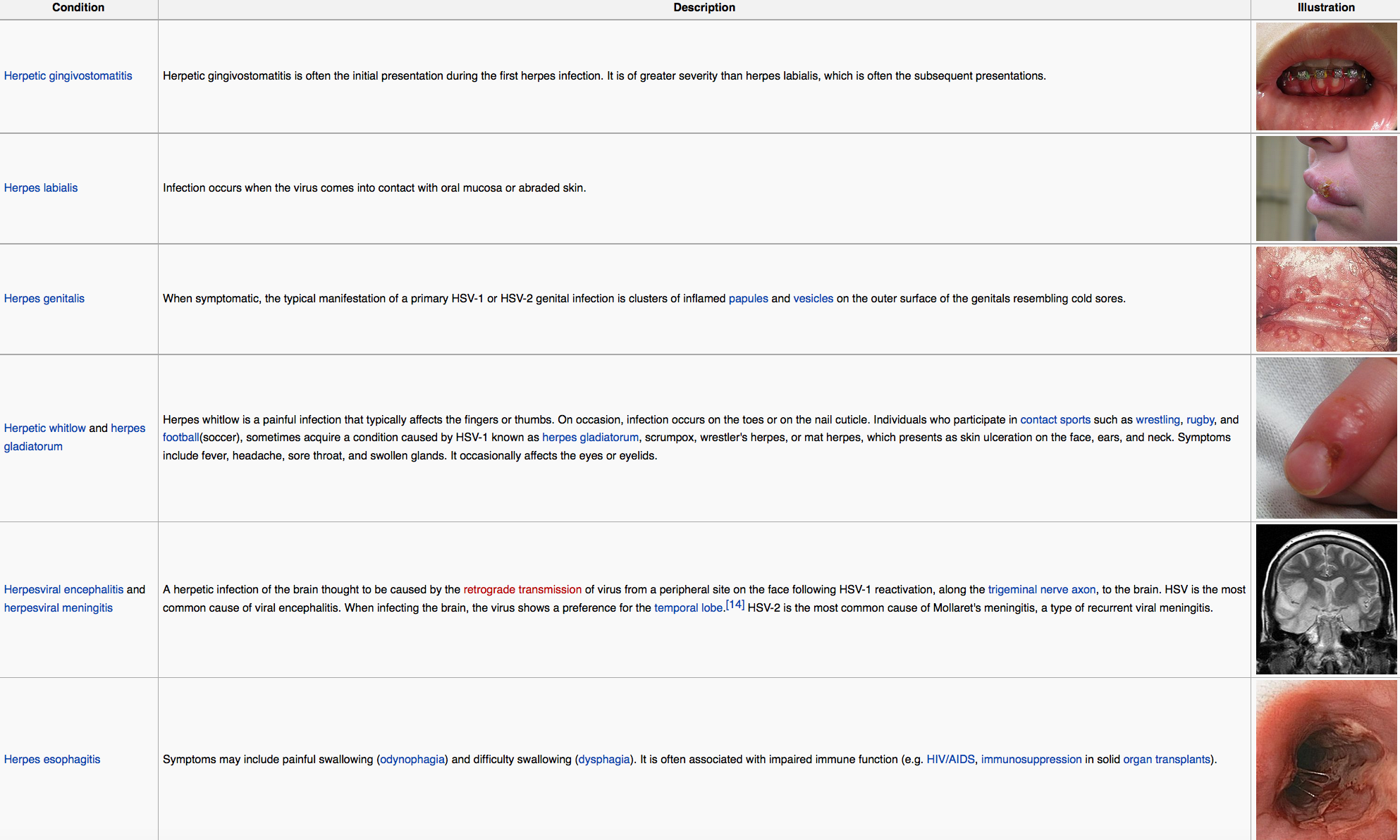
HSV infection causes several distinct medical disorders. Common infection of the skin or mucosa may affect the face and mouth (orofacial herpes), genitalia (genital herpes), or hands (herpes whitlow). More serious disorders occur when the virus infects and damages the eye (herpes keratitis), or invades the central nervous system, damaging the brain (herpes encephalitis). Patients with immature or suppressed immune systems, such as newborns, transplant recipients, or AIDS patients are prone to severe complications from HSV infections. HSV infection has also been associated with cognitive deficits of bipolar disorder,[2] and Alzheimer's disease,[3] although this is often dependent on the genetics of the infected person.
In all cases HSV is never removed from the body by the immune system. Following a primary infection, the virus enters the nerves at the site of primary infection, migrates to the cell body of the neuron, and becomes latent in the ganglion. As a result of primary infection, the body produces antibodies to the particular type of HSV involved, preventing a subsequent infection of that type at a different site. In HSV-1 infected individuals, seroconversion after an oral infection will prevent additional HSV-1 infections such as whitlow, genital herpes, and keratitis. Prior HSV-1 seroconversion seems to reduce the symptoms of a later HSV-2 infection, although HSV-2 can still be contracted. Most indications are that an HSV-2 infection contracted prior to HSV-1 seroconversion will also immunize that person against HSV-1 infection.[citation needed]
Many people infected with HSV-2 display no physical symptoms—individuals with no symptoms are described as asymptomatic or as having subclinical herpes.
 Bell's palsy
Bell's palsy
Although the exact cause of Bell's palsy, a type of facial paralysis, is unknown it may be related to reactivation of herpes simplex virus type 1. This theory has been contested, however since HSV is detected in large numbers of individuals who never experienced facial paralysis, and higher levels of antibodies for HSV are not found in HSV-infected individuals with Bell's palsy compared to those without. Regardless antivirals have been found to not improve outcomes.
Alzheimer's disease
SV-1 has been proposed as a possible cause of Alzheimer's disease.[ In the presence of a certain gene variation (APOE-epsilon4 allele carriers), HSV-1 appears to be particularly damaging to the nervous system and increases one’s risk of developing Alzheimer’s disease. The virus interacts with the components and receptors of lipoproteins, which may lead to the development of Alzheimer's disease. Without the presence of the gene allele, HSV type 1 does not appear to cause any neurological damage and thus increase the risk of Alzheimer’s. Herpes simplex virus type 1 DNA is localized within the beta-amyloid plaques that characterize Alzheimer's disease. It suggests that this virus is a major cause of the plaques and hence probably a significant aetiological factor in Alzheimer's disease.
Pathophysiology
Herpes is contracted through direct contact with an active lesion or body fluid of an infected person. Herpes transmission occurs between discordant partners; a person with a history of infection (HSV seropositive) can pass the virus to an HSV seronegative person. The only way to contract Herpes simplex virus 2 is through direct skin-to-skin contact with an infected individual.[citation needed] To infect a new individual, HSV travels through tiny breaks in the skin or mucous membranes in the mouth or genital areas. Even microscopic abrasions on mucous membranes are sufficient to allow viral entry.
HSV asymptomatic shedding occurs at some time in most individuals infected with herpes. It can occur more than a week before or after a symptomatic recurrence in 50% of cases. Virus enters into susceptible cells via entry receptors such as nectin-1, HVEM and 3-O sulfated heparan sulfate. Infected people that show no visible symptoms may still shed and transmit virus through their skin; asymptomatic shedding may represent the most common form of HSV-2 transmission. Asymptomatic shedding is more frequent within the first 12 months of acquiring HSV. Concurrent infection with HIV increases the frequency and duration of asymptomatic shedding. There are indications that some individuals may have much lower patterns of shedding, but evidence supporting this is not fully verified; no significant differences are seen in the frequency of asymptomatic shedding when comparing persons with one to twelve annual recurrences to those who have no recurrences.
Antibodies that develop following an initial infection with a type of HSV prevents reinfection with the same virus type—a person with a history of orofacial infection caused by HSV-1 cannot contract herpes whitlow or a genital infection caused by HSV-1. In a monogamous couple, a seronegative female runs a greater than 30% per year risk of contracting an HSV infection from a seropositive male partner.[24] If an oral HSV-1 infection is contracted first, seroconversion will have occurred after 6 weeks to provide protective antibodies against a future genital HSV-1